
Breast implant surgery sometimes requires revision soon after the initial operation due to problems with either implant size or implant position. Over time, revision becomes necessary when excessive scar tissue forms around the implant or when the implant breaks or ruptures. The exact procedure done depends on the particular situation. Contact our Dallas office to schedule your breast implant revision consultation.
Reasons Why Women Undergo Early Breast Implant Replacement Surgery
Misplaced Implants
Following breast implant surgery, some implants are too high on the chest. This can be due to the implant being placed too high at surgery, it can be from pectoralis muscle contraction displacing the implant, or it can be caused by early scar tissue formation around the implant. Surgery to correct this is relatively simple and involves making the implant pocket lower so the implant moves down.
Alternatively, implants can be too low. When occurring early after surgery, it is usually due to surgical technique. When it occurs later, it is more frequently due to the weight of the implant stretching out of the patient's tissues. This is sometimes called "bottoming out," and it is most commonly seen with saline breast implants. This situation is more difficult to treat as it involves working against gravity. Here, the surgeon has to reduce the size of the implant pocket so as to elevate the implant. Recurrence is a real problem in this situation. Dallas breast implant revision surgeon Paul Pin frequently will encourage the patient to use silicone implants when the implant is too low as silicone implants are much less likely to cause stretching and recurrence of the problem.
Implant Size Problems
Despite the best efforts of the surgeon, patients are occasionally dissatisfied with their breast size post-operatively. This commonly results when a patient chooses her implant size pre-operatively by placing an implant in her bra. The implant will always look smaller once it is inserted, especially when it is placed beneath the pectoralis major muscle. Additional problems can arise when the goal of surgery is to create a certain cup size. Breast implants come in volumes (for instance, one 270cc implant is 9 fluid ounces) and have no consistent relationship with cup size. As much as possible, Dr. Pin tries to refrain from promising a certain post-operative cup size.
Regardless of cause, a change in implant size requires surgery to place a new implant. An exception is when a saline implant is inflated further. While this is minimally invasive and inexpensive, it usually results in an excessively firm implant and is therefore not commonly done.
Occasionally, the cause of a woman being too large after an augmentation is that her breast has actually gotten bigger. While this takes time to occur, it can happen as a result of weight gain, hormone treatment, pregnancy, or simply aging. Women in this situation may choose to downsize their implants or remove them altogether.
When Dr. Pin sees a patient who feels she has the wrong size implant, he spends a great deal of time going over pictures of other patients so as to determine her goal. Dr. Pin also tries to emphasize the importance of measurements besides volume, such as the width and projection of the implant.
Featured Cases

Breast Implant Revision with Silicone Implants
This 35 year old desired revision of her deflated saline implants, which she felt were too large.
+ See Full Case
Breast Implant Revision with Silicone Implants
This 22 year old desired an augmentation revision. She was 5'4", weighed 127 pounds, had 440 cc saline implants and wanted to be smaller.
+ See Full CaseReasons Why Women Undergo Late Breast Implant Replacement Surgery
Capsular Contracture
Capsular contracture or the apparent hardening of the breast implant is due to the formation of excessive scar tissue around the implant. This scar tissue reduces the mobility of the implant, gives the breast an unnatural appearance and feel, and can even cause significant discomfort. While at one time this problem was extremely common, surgery to treat this condition is now necessary in less than 5 percent of patients. This dramatic reduction is attributable to better implants, more careful surgical technique, and better infection prevention.
The treatment of capsular contracture involves surgery to remove surrounding scar tissue. If the implant is on top of the pectoralis major muscle, Dr. Pin will almost always move it beneath the muscle, as this is associated with a lower risk of recurrent contracture. While in this situation, some plastic surgeons will use breast implants with textured surfaces, Dr. Pin?s own experience is that these implants are more likely to develop recurrent contracture, and so he seldom uses them.
Implant Rupture
Breast implants, like any other product, eventually wear out and break. Saline breast implant failure is associated with the slow or sudden loss of breast volume and is usually very obvious to the patient. Silicone implant rupture is more difficult to identify because the silicone gel largely remains in the pocket around the implant. While some patients may report a change in breast consistency, either firmer or softer, the majority of silicone implant failures are "silent" and have to be identified by breast ultrasound, mammography, or MRI.
When a saline implant leaks, it is usually on one side and causes significant asymmetry, which prompts a patient to seek surgery to correct the problem. Because silicone implant rupture does not usually cause a cosmetic problem, surgery is usually less urgent. The FDA and most plastic surgeons recommend that patients with ruptured silicone implants have surgery to remove their implants. This is largely because some patients will have small amounts of silicone migrate into their breasts and lymph nodes. This can result in lumps that are painful and difficult to treat. These lumps can also mimic breast cancer and make breast self-examination difficult.
When Dr. Pin sees a patient with a ruptured silicone implant, he tries to help them decide if they should replace their implant. Patients who have been happy with their implants should consider replacement. Patients who have never really been happy with their implants should avoid replacing them unless the revision can substantially improve on the previous outcome. Some patients have a hard time deciding what to do and are concerned about what they will look like without implants. In this group, if Dr. Pin knows their implant size, he can usually give them an idea of their cup size without implant, and this greatly facilitates their decision. Patients who are worried about being ptotic or droopy after their implant removal can be offered a mastopexy or breast lift at the same time to ensure better breast shape post-operatively.
DESIRE TO CONVERT FROM SALINE TO SILICONE
Numerous patients these days who are interested in replacing their aging saline implants. While some choose to place new saline implants, many are interested in switching to silicone. There are several motivations for the change, but here are a few:
Better Quality Implant Due to viscosity of the silicone compared to saline, a silicone implant results in a breast that feels much more natural. Additionally, silicone implants have much fewer problems with visible and palpable rippling. Diminished rippling is most likely to be seen when a patient moves from a textured saline implant to a smooth silicone implant.
Implant Malposition The most common, long-term problem with saline implants is that they stretch out the patient’s breast tissue and the implant ends up too low and too far out to the side. This is most bothersome to patients whose original motivation for the procedure was to restore fullness in the upper part of their breasts. With stretching of the lower part of the breast, patients lose their upper breast volume and end up having the same, “droopy” shape they started with, only now they are bigger.
With stretching of the side of the breast, patients notice migration of their implants to the side (or even off their chests) when they lie down. Problems related to stretching of the breast from saline implants can usually be treated with revisional surgery and conversion to a silicone implant. Because silicone is “thicker” or more viscous than saline, there is considerably less tendency for the implant to stretch the patient’s breast. As a result, the implant position is much more stable over time.
DESIRE TO CHANGE IMPLANT SIZE
Some patients may have implants that are just too small and want to move to a larger implant. This typically occurs in a woman who had an augmentation prior to pregancy and then lost native breast volume after the pregnancy. This is the simplest type of revision and has a high degree of patient satisfaction.
Alternatively, as some women age, the overall size of their breasts may become too large. This can result from a combination of weight gain, hormone treatment, pregnancy, or simply aging. Some women feel they should have, "age appropriate breasts," and feel a size that is great in one's thirties is less attractive in one's fifties> Women in this situation may choose to downsize their implants or remove them altogether. When making this decision it is important to have as much information as possible about the current implant type, volume and shape. Implant position is also very important as an implant placed above the muscle will frequently make the central breast concave if removed completely. While some of this can be mitigated by a breast lift, complete implant removal can sometimes result in a less than attractive breast. A thorough physical examination and review of the implant characteristics will usually allow the surgeon to give the patient realistic expectations.
Breast Implant Revision Procedure
Breast implant revisional surgery usually takes less than two hours and is done under general anesthesia as an outpatient. Sutures are always dissolvable, there are no bandages, and showing may resume the following day. Unlike breast augmentation, drains are sometimes used in revisional surgery. In a simple implant exchange where the size or the type of implant is being altered, drains are never used. Drains may be used if the implant pocket is being changed, usually from subglandular to sub muscular, or if there is a significant capsular contracture. Drains are used with pocket change to prevent fluid from accumlation at the old site which can prevent healing of the pocket. In contracture treatment, the operated breast will frequently ooze considerably after surgery, which has two negative consequences. The first is the fluid accumulation will cause significant discomfort, while the second is the fluid will contain stem cells that make it more likely for the contracture to recur. If drains are used, they are usually left in place for only a day or two and removal is almost always painless.
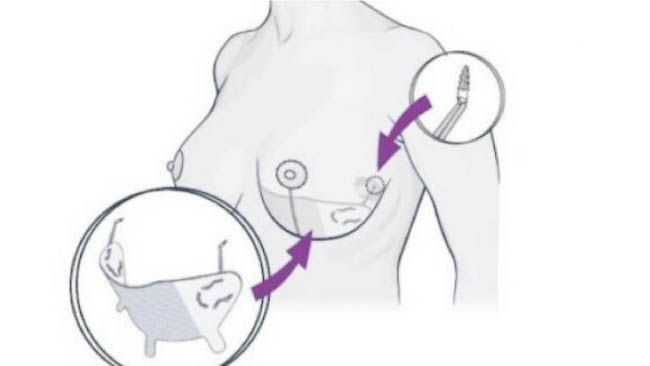
GALAFLEX MESH FOR IMPLANT REVISIONS
Some revisions are more complicated than others and require newer techniques. An example of a difficult revision is when an implant is too low or too far laterally. This happens frequently when patient had a saline implant for many years or when a patient has an implant heavier than their tissues can support. The standard way to reposition an implant is with a “ capsulorrhaphy” where the scar around the implant, the capsule, is sutured at a higher level to support the breast implant. No matter how this procedure is done, it fails about 50% of the time, and the implant returns to its prior position.
Fortunately, there is a solution to this problem by using a surgical mesh call Galaflex. While “mesh” has many negative associations for patients, Galaflex is different. Many meshes that cause problems are usually made of a permanent, plastic material that can be associated with severe scarring or infection. Other meshes like Alloderm or Strattis come from deceased humans or pigs. These meshes, called acellular dermal matrix (ADM), have a high infection rate and are obscenely expensive. (A 6 X 4 inch piece of Alloderm can cost over $3,000.)

Galaflex is an “organic” mesh that works as a scaffold for new tissue growth, which is rapidly vascularized and becomes fully integrated with adjacent tissue. (See image above.) The lattice that is formed acts as an “internal bra” to support the new implant position. Then, unlike other surgical mesh, Galaflex dissolves and is usually gone within 6-12 months. Therefore, there are no long-term complications as with other meshes. Compared with other alternatives, Galaflex is much less expensive, has a much lower infection rate, and most importantly, it works predictably to maintain a new implant position. (See image below.)
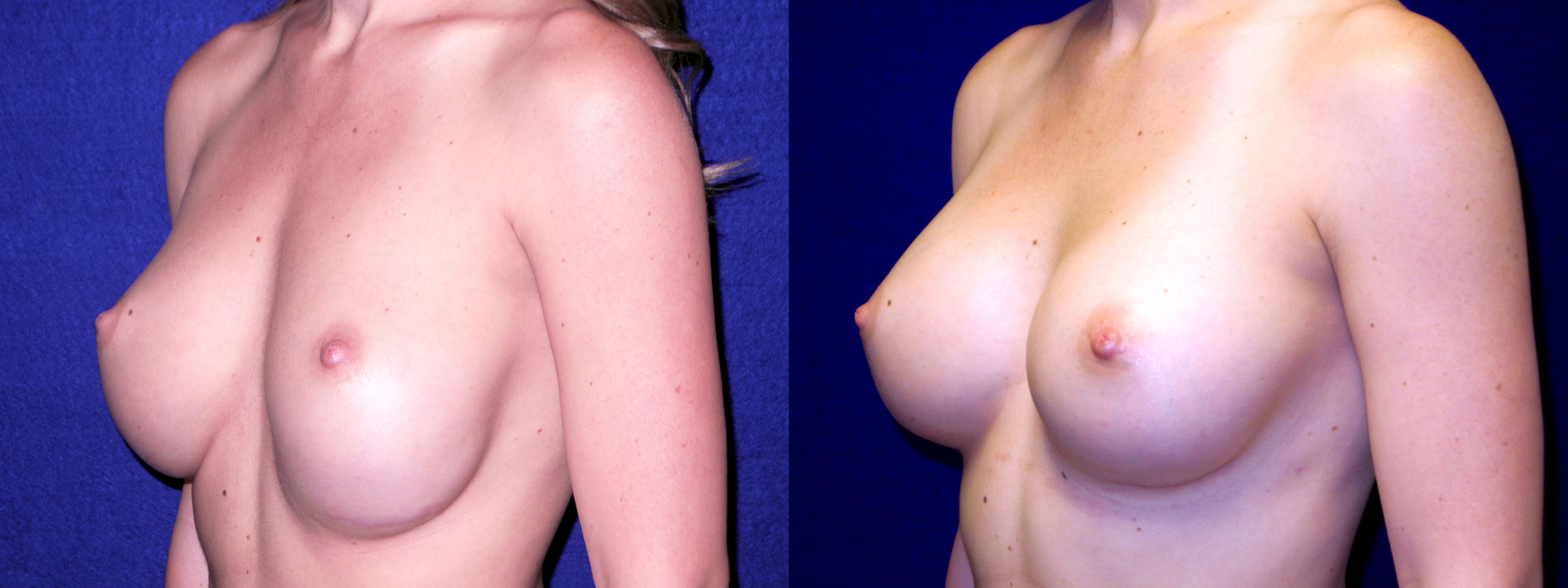
The patient below had a previous augmentation and her implant settled in too low a position. A revision was performed using Galaflex, which resulted in successful repositioning her implant.
Galaflex is also useful in other surgical situations. For instance, it can be used to prevent the development of implant malposition, which is a common concern with implants over 400 cc. Additionally, it can be employed during a breast lift or reduction to maintain the patient’s breast shape and prevent recurrent drooping of the breast.
Dallas Breast Implant Revision Consultations
While all breast implant revisions require surgery, most patients find it to be not that difficult, and virtually all procedures are done on an outpatient basis. In most situations, patients can return to work within a week and return to normal activity shortly thereafter. Regardless of what is done, most revisions result in a tremendous improvement for the patient. Contact our Dallas office today to schedule your breast replacement surgery consultation.
Breast implant revision is real surgery and involves risks such as bleeding, infection, and scarring. Results vary. Dr. Pin will be happy to discuss these and other risks of breast implant revision.